Basal Ganglia Hemorrhage
What is basal ganglia hemorrhage?
The basal ganglia hemorrhage can be defined as a form of hemorrhage that occurs inside the brain, being primarily caused by a hypertension that was poorly kept under control. The patients who suffer from this form of hemorrhage also present the signs of chronic hypertensive encephalopathy. It is important to remember that the hemorrhages caused by hypertension can appear in other areas of the brain as well, such as the pons or the cerebellum.
When a bleeding occurs at the level of the basal ganglia, this means that the area of the brain that is responsible for the movements of the body, sensation, speech and personality has suffered. The basal ganglia hemorrhage is one of the most frequent hemorrhages that occur at the level of the brain. The accumulation of blood at the level of the brain can actually lead to compression, followed by the damage of the brain tissue. High blood pressure remains the main cause why the arteries at the level of the basal ganglia burst, leading to hemorrhage.
Anatomy of the Basal ganglia (in Pictures)
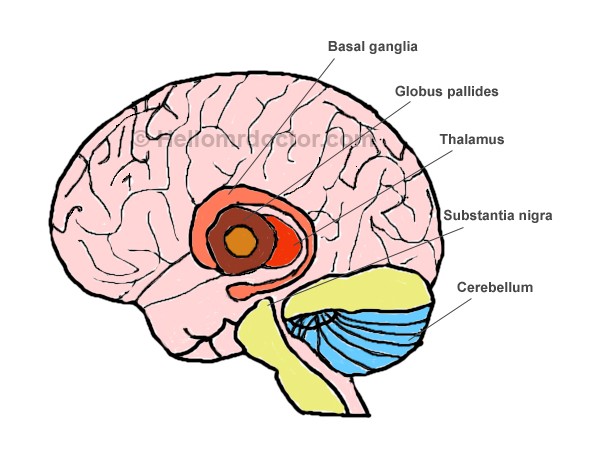
Picture 1 showing Basal ganglia and related structures of the brain : Globus pallidus, Basal ganglia, Thalamus, Substantia nigra and Cerebellum.
Pathophysiology
If a person suffers from chronic hypertension and this is not properly kept under control, this will lead to a number of pathological changes at the level of the blood vessels (including those at the level of the brain).
Microaneurysms can occur at the level of perforating arteries, these being also known as the Charcot-Bouchard aneurysm. These have a small diameter, often occurring on arteries that are small in diameter as well. Upon a close analysis, it seems that the microaneurysms have a similar location with the actual hypertensive hemorrhage – 80% lenticulostriate, 10% pons and 10% cerebellum. These are found in patients who suffer from chronic hypertension – it is possible that they thrombose or rupture. In case of leakage, the patient can suffer from what is known as a cerebral microhemorrhage.
Apart from the microaneurysms, it is possible that the larger vessels are affected by the atherosclerosis process. Arteriosclerosis is present in two different forms, meaning the hyaline and the hyperplastic ones. The latter is most often encountered in severe cases.
The basal ganglia is a very important of the brain, being located at the level of the cerebrum and playing an essential role in the following areas: cognitive function, eye movement, procedural learning and motor control. There are three major functions that the basal ganglia is responsible of, meaning: suppression of undesired movements, regulation of muscle tone and movement control (the basal ganglia contributes to the initiation and termination of body movements).
While the hypertension is known as a precipitating factor, there are other factors that are known as “predisposing”. Among these factors, there are: leading a sedentary lifestyle, eating an unhealthy diet, age, gender, hereditary and choosing self-medication. Due to all of these factors, a chronic process of vasoconstriction appears. This in turn leads to the blockage of the blood vessels, with a reduction in the oxygen and nutrient supply. Once the brain does not receive what it needs, the cerebral perfusion is going to be altered and reduced. The alteration of the perfusion is responsible for the basal ganglia hemorrhage, with the blood irritating both the nerves and the tissues in the area.
It is also possible that, due to the basal ganglia hemorrhage, a blood clot will form in the area. This will cause the compression of the brain tissues in the area, with the patient suffering from specific symptoms.
Symptoms
The symptoms caused by the basal ganglia hemorrhage are present at different levels, as you will have the opportunity to see below:
Body movement
- Difficulties swallowing, smiling or speaking
- Ataxia
- Tremor
- Loss of movement/rigid movements
- Paralysis or hemiparesis
Cognitive function
- Difficulties in processing information or taking decisions
- Memory problems (memory loss, forgetfulness)
- Language difficulties (spoken and written)
- Attention deficit or short span of attention
Vegetative symptoms
- Nausea and vomiting
- Headaches
- Loss of consciousness (various degrees)
Changes in relation to the personality
- The patient presents difficulties in understanding information
- Frustration or anxiety
- No longer feels motivated, losing the interest for daily activities or work
- Mood swings – laughs or cries for no reason
- Feelings of depression or anger.
Diagnosis
These are the most common used methods for the diagnosis of the basal ganglia hemorrhage:
Imaging studies
- CT scan
- Hyperdensity identified at the level of the basal ganglia or thalamus
- The hemorrhage can extend to the brain ventricles (small parenchymal component)
- MRI
- Identification of the hemorrhage that has occurred at the level of the basal ganglia.
Treatment and Prognosis
In general, one of the main objectives of the treatment is keeping the hypertension under control, in order to prevent the basal ganglia hemorrhage in the future. If the hemorrhage has occurred, with hydrocephalus being also present at the level of the brain, CSF drainage might be required (along with the extra-ventricular drain). The evacuation of the clot is only recommended only in the large hemorrhages (over 60 ml). Pain medication can be administered to bring the necessary pain relief (often the pain appears as the result of immobilization).
Physical therapy is essential during the recovery period for the patient. It is based on exercises that are meant to strengthen the muscles and also on movements destined to increase the range of motion. The physical therapist will include exercises that are both active and passive; some of them will concern the improvement of the balance and coordination, while others address the problems related to sensory organization. Locomotion training is going to be performed, with or without walking aids or other specialized equipment. Some patients might need to learn how to use a wheelchair – the physical therapist will also provide assistance when it comes to making the necessary transfers. The occupational therapist will work hand in hand with the physical therapist – he/she will be responsible for teaching the patient how to handle the activities of daily living with the current abilities.
