Oncocytoma
What is Oncocytoma?
Oncocytoma can be described as a tumor that is mainly constituted out of oncocytes. These are actually epithelial cells, containing excessive quantities of mitochondria. This excess leads to a cytoplasm that is acidophilic and granular. It is important to understand that the cells comprising the oncocytoma are benign in nature; however, there are patients in which these cells demonstrate a pre-malignant or malignant state (malignant transformation).
Histopathology
The oncocytes that contribute to the formation of oncocytoma are epithelial cells, as it was already mentioned. The composition of oncocytoma is what places it in the epithelial tumors category. The oncocytes are eosinophilic cells that are large in size, having a small and round nucleus. They nucleus has a benign appearance, being surrounded by nucleoli that are large in size as well. One should keep in mind that the oncocytoma is not restricted to a particular organ; on the contrary, it can arise in more than just one organ.
Renal oncocytoma
Despite being a benign tumor, it is quite difficult for it to be distinguished from the renal cell carcinoma. The renal oncocytoma is one of the primary adult epithelial renal neoplasms that are treated through surgical resection (5% of all the cases). The condition often affects patients who are in their 6th-7th decade of life, with the peak incidence being at approximately 55 years.
The male population is predisposed to developing this condition, with the majority of the patients being asymptomatic. If a large mass occurs in the flank or abdominal area, the patient might start to present symptoms – pain is the most common complaint. Apart from pain, the patient can present blood in the urine (hematuria) or occasional high blood pressure (hypertension). This condition can be found in association with other medical problems, such as the Birt-Hogg-Dubé syndrome or the tuberous sclerosis.
Pathology
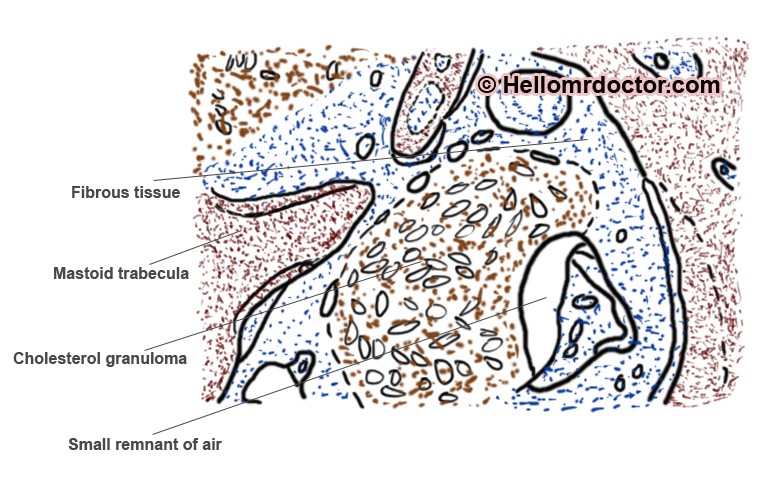
The growths that are larger in size present a tan color, which is similar to the one of the renal cortex. In some situations, the macroscopic oncocytoma might appear to be darker in color. A pseudocapsule can be present in some of the growths. It is also possible that macroscopic hemorrhage appears (20% of all the cases). It is not helpful to perform a biopsy on the oncocytoma, hoping to make the differential diagnosis from the renal cell carcinoma (as this contains oncocytic elements as well). Necrosis is not present.
Diagnosis
These are the most common methods used for the diagnosis of the renal oncocytoma:
- Imaging studies
- Sharp and demarcated lesions of various sizes
- Difficult to distinguish from renal cell carcinoma (due to the similar appearance)
- Sharp central stellate scar – helpful sign, characteristic of oncocytoma (only in 1/3 of the cases)
- May reveal the metastasis or the aggressive infiltration of the adjacent structures (the diagnosis if then of renal cell carcinoma)
- Both kidneys have to be evaluated – patients can present multiple oncocytomas in both kidneys; moreover, concurrent renal cell carcinomas can be identified
- Intravenous pyelogram
- Sharp demarcation of the growths
- Enhancement is noticed during the nephrographic phase
- Ultrasound
- Well-circumscribed mass
- Central scar might be visible (not in all patients)
- CT
- Large and well-demarcated tumors identified
- Can be made with non-contrast and contrast
- MRI
- Typical characteristics present, including the central stellate scar
- Angiography
- Spoke wheel pattern identified – the peripheral vessels are penetrating into the center of the lesion
- The investigation can also serve to the identification of the microaneurysms in the area.
Based on the available imaging studies, the differential diagnosis can be made with the following conditions: renal cell carcinoma (very difficult to be made, due to the highly similar characteristics), metanephric neoplasms (adenoma or adenofibroma) and renal leiomyoma.
Treatment and prognosis
The surgical resection is often the first line of treatment for the renal oncocytoma, as these lesions cannot be clearly distinguished from the renal cell carcinoma. Renal sparing surgery is performed only in the situation that the diagnosis is confirmed pre-operatively.
Salivary gland oncocytoma
Also known as the oxyphilic adenoma, this is a benign neoplastic growth that occurs at the level of the salivary glands. The tumor is well-circumscribed and it represents approximately 1% of all the tumors affecting this particular part of the body. Upon performing a histopathological analysis, inflamed oncocytes are going to be revealed (the cells contain excessive quantities of mitochondria).
This form of oncocytoma is often encountered in patients of older age (70-80 years). The oncocytoma is more commonly identified at the level of the parotid gland (85-90% of the cases). The growth is firm and painless, growing on a gradual, slow manner. The diameter of the mass is under 4 cm. A bilateral presentation is often encountered with the salivary gland oncocytoma.
Thyroid oncocytoma
The thyroid oncocytoma can appear either a benign (adenoma) or a malignant (carcinoma) growth. In the situation that the growth is benign, it will take the form of an encapsulated and solid nodule. More than one nodule can be present, all of them having a characteristic, brown cut surface. When it comes to the malignant growths, there are not many things that distinguish it from a benign lesion. A trained eye can recognize the invasion of the cancerous cells in the healthy tissue, as well as the development of the vascularization in the area (neo-vascularization). The transcapsular and/or vascular invasion remain the main criteria used for the diagnosis of the malignant thyroid oncocytoma.
The patients who suffer from thyroid oncocytoma generally present a thyroid nodule, with the rest of the thyroid gland functioning normally. When the tumor becomes too large in size, invading the area around the thyroid gland, the patient might experience difficulties swallowing or talking.
In conclusion, the general treatment for oncocytoma is represented by the surgical resection. This guarantees the best outcome for the patient and also the relief from the experienced symptoms, if any. As you have had the opportunity to read, the renal oncocytoma presents the most complex diagnostic difficulties, as it shares many of its characteristics with the renal cell carcinoma.